Trigger Finger
What is it?
Trigger finger is a condition where the normal and smooth motion of a finger or thumb flexion is compromised. It is a very common condition and is often painful.
What are the symptoms?
Trigger finger usually results in a finger that catches, locks, or sticks as it tries to move. This typically presents as a finger that cannot easily open from a flexed position, but sometimes presents as a finger that is completely stuck in a flexed position or one that cannot flex all the way. Additional effort, such as forceful extension or the use of the other hand, is often required to overcome impediment to motion. Symptoms are often worse in the morning.
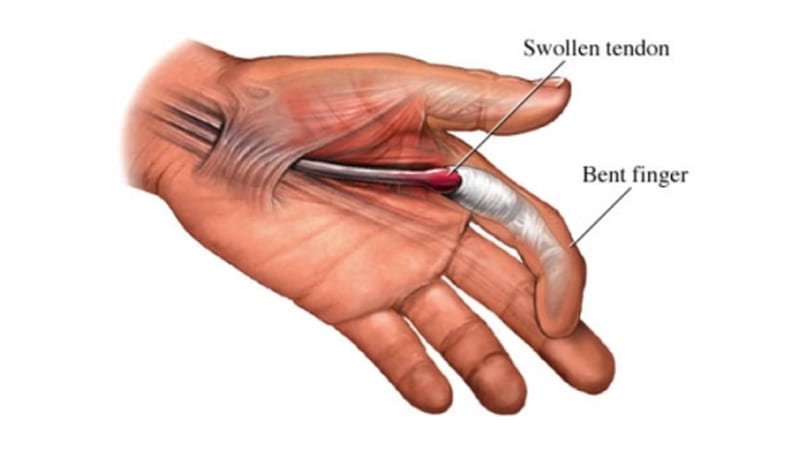
What causes it?
Trigger finger occurs when the flexor tendons that move the fingers are unable to easily pass through the tendon sheaths that they travel through. Tendon sheaths are necessary to restrain the tendons against the bone, preventing the tendons from bowstringing when the finger moves and thus improving the tendon’s efficiency. At the area of the first pulley, the A1 pulley, the tendons and pulley system are subjected to higher stresses, with the result that inflammation, thickening or fibrosis may occur. This impedes the smooth excursion of the tendons and can result in pain and triggering. The cause of the condition is typically iatrogenic, meaning no cause is readily identifiable. Sometimes other conditions, such as diabetes or carpal tunnel syndrome, make trigger fingers more likely to occur.
Diagnosis:
A simple physical examination is sufficient to diagnose a trigger finger and rule out other conditions that mimic it.
What is the treatment?
Many conservative treatments for trigger finger are available. Splinting of the digit may prevent triggering at night. Therapy is not typically effective. Steroid injections into the sheath or overlying tissues has been shown to be successful, although recurrence is common. Repeat steroid injections can be performed. Surgical management involves the release of the A1 pulley which removes the focal area of constriction and eliminates the triggering. This is usually accomplished via an incision in the palm overlying the pulley. Additionally release of the tendon sheath can also be done with a needle through the skin. Early range of motion and activity is encouraged after surgery.
Are you ready to get treated? Book your appointment here.